Definition of innovative medicine
The candidate list of innovative medicines in the Hong Kong setting was generated from horizon scanning conducted up to 31 December 2024. Only those medicines with Phase III trial evidence were considered eligible for inclusion and were subsequently included in this analysis.
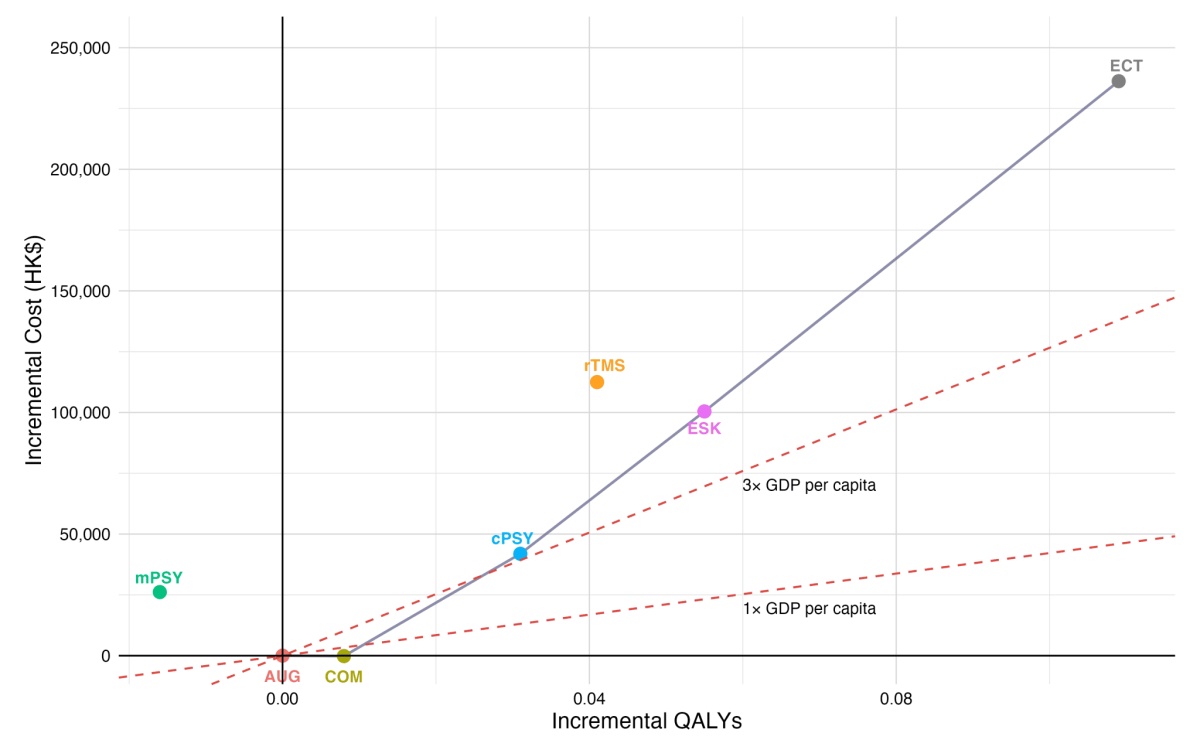
The cost-effectiveness frontier included AUG, COM, cPSY, ESK, and ECT. This indicates that these strategies were non-dominated options in the incremental cost-effectiveness analysis. Compared with AUG, ESK had an ICER of HK$1,825,149 per QALY. This exceeded the WTP threshold of three times GDP per capita in Hong Kong (HK$1,265,970 per QALY).
Note:
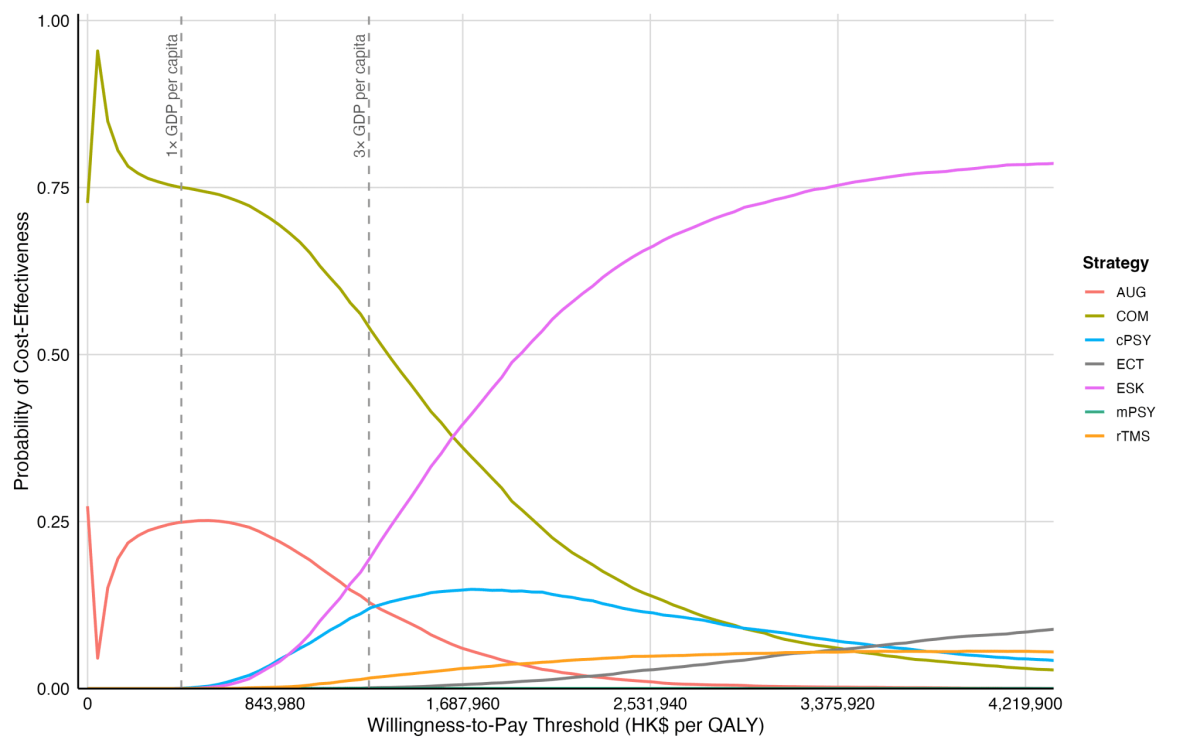
The cost-effectiveness acceptability curves summarise uncertainty in cost-effectiveness across different WTP thresholds. At the threshold of three times GDP per capita in Hong Kong, HK$1,265,970 per QALY, ESK had a 19.3% probability of being the most cost-effective strategy, while COM remained the preferred option. At a higher WTP threshold of HK$1,643,347 per QALY, ESK became the most likely cost-effective option.
Note:
Abbreviations: AUG, augmentation therapy (antidepressant combined with antipsychotic/lithium); COM, combination therapy (antidepressant combined with antidepressant); mPSY, psychotherapy alone; cPSY, psychotherapy combined with antidepressant; ESK, esketamine combined with antidepressant; rTMS, repetitive transcranial magnetic stimulation combined with antidepressant; ECT, electroconvulsive therapy combined with antidepressant; GDP, gross domestic product; QALY, quality-adjusted life year; WTP, willingness-to-pay.
The target population comprised patients with treatment-resistant depression (TRD) in Hong Kong, identified from the territory-wide electronic medical database managed by Hong Kong Hospital Authority. At model entry in 2024, the baseline prevalent population was 7,678 patients. The annual incident cohorts entering the budget impact model in 2025–2029 were projected to be 578, 969, 1,228, 1,238, and 1,247, respectively.
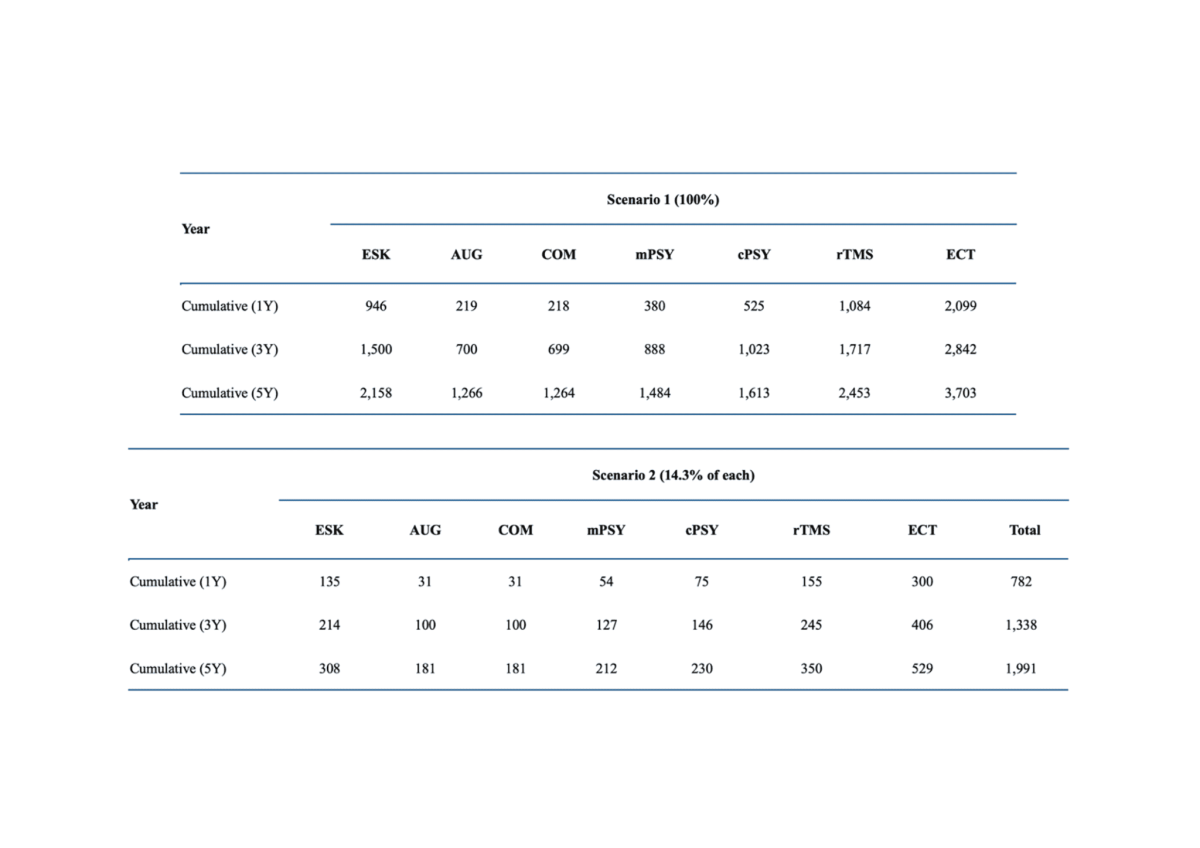
Two market share scenarios were assessed to illustrate a range of possible uptake for each treatment strategy among patients in the treatment pathway.
Abbreviations: TRD, treatment-resistant depression; AUG, augmentation therapy (antidepressant combined with antipsychotic/lithium); COM, combination therapy (antidepressant combined with antidepressant); mPSY, psychotherapy alone; cPSY, psychotherapy combined with antidepressant; ESK, esketamine combined with antidepressant; rTMS, repetitive transcranial magnetic stimulation combined with antidepressant; ECT, electroconvulsive therapy combined with antidepressant.

